Volume 10 Issue 1 pp. 17-30 • doi: 10.15627/jd.2023.2
Visual Comfort Assessment of Hospital Patient Rooms with Climate Responsive Facades
Horre Toodekharman,⁎ Mahdieh Abravesh, Shahin Heidari
Author affiliations
Department of Architecture, University of Tehran, Tehran, Iran
*Corresponding author.
toodekharman@ut.ac.ir (H. Toodekharman)
abravesh@ut.ac.ir (M. Abravesh)
shheidari@ut.ac.ir (S. Heidari)
History: Received 11 January 2023 | Revised 17 February 2023 | Accepted 21 February 2023 | Published online 12 March 2023
Copyright: © 2023 The Author(s). Published by solarlits.com. This is an open access article under the CC BY license (http://creativecommons.org/licenses/by/4.0/).
Citation: Horre Toodekharman, Mahdieh Abravesh, Shahin Heidari, Visual Comfort Assessment of Hospital Patient Rooms with Climate Responsive Facades, Journal of Daylighting 10 (2023) 17-30. https://dx.doi.org/10.15627/jd.2023.2
Figures and tables
Abstract
As advanced technologies become prevalent, they are being used more widely in numerous fields. The building sector is not an exception. One of these cutting-edge technologies is responsive facades, which are used in buildings and have an undeniable effect on daylighting. However, they have not been adequately evaluated for improving visual comfort in hospitals. This study investigates visual comfort in a standard patient room, based on applying four responsive facades. Simulations were conducted using HoneybeePlus, a plugin in the Grasshopper. Simulation-based results of annual indicators, including Annual Sunlight Exposure (ASE) and spatial Daylight Autonomy (sDA), showed that different facades could result in several optimal modes. Furthermore, a more comprehensive investigation should consider factors such as Daylight Glare Probability (DGP) and Daylight Glare Index (DGI). Glare indicators revealed that facade directly affects patient visual comfort and can even have an adverse effect. When the optimal responsive facade is chosen, it enhances users' visual comfort throughout the year, yet there will be still glare probability in some cases. Based on the results, this probability decreases as patient distance increases, and Window to Wall Ratio (WWR) is not particularly effective in reducing glare. Nevertheless, when it comes to daylight availability, WWR cannot be ignored, and the first façade with WWR 60% showed the best overall performance.
Keywords
Responsive façade, Visual comfort, Patient room, Glare probability
1. Introduction
As a member of the modern world, applied technologies have a significant role to play in various topics. For example, construction technologies are increasingly growing, and new buildings are turning to the use of advanced techniques and sustainable materials [1]. Different parts of the building can be updated according to available technologies, as well as other parameters such as its impact on energy consumption and user comfort. The building envelope is one of the main parts of the building that is constantly exposed to the climatic conditions, so it is better to have the ability to adapt to the changes. Heat transfer occurs through the envelope, and in addition to user comfort, it has a direct effect on cooling and heating energy consumption [2]. Besides examining thermal characteristics, the facade should also be evaluated from an aesthetic standpoint. A good example is Origami, which inspires facade designers and has been studied from a daylighting and energy perspective many times [3,4]. Another inspiration source for facade design is nature, where each element can have its unique characteristics and can be adapted to the climate [5]. Due to the frequent development of facade technologies, another design option is to use a responsive facade in adaptive buildings [6]. Responsive facades can be categorized from various aspects, such as control type and scale [7]. They have the same functional features as smart facades, perform real-time perception, component mobility, building automation, and user-centric operations, and have intelligent materials. Still, it is also an interactive facade because it can learn automatically, through the gradual education of the building and its occupants [8]. A parametric design can also make it more beautiful as well as perform better. The parametric facade provides a broad view of multiple solutions to architectural design problems using algorithmic methods [9]. However, it has been stated that the key reason for not using these mechanical facades is the lack of a controllable substitution in times of need [10].
Studies have shown the frequent examination of responsive facades in office buildings. These studies were based on various aspects, such as interactive 2D and 3D kinetic facades with the capability to be transformed based on dynamic daylight [11]. Another novel example is using adaptive reflective façade for a single floor office [12]. Finding the best pattern for the façades of the open-plan office buildings is another research subject in terms of visual comfort [13]. By optimizing the façade design parameters, including perforation ratio, depth, and the gap width from the outer wall, office environments become more visually comfortable [14]. Office buildings could have some additional spaces such as atriums, which contribute significantly to sustainable architecture [15]. This is a passive architectural element and passive design is investigated in other building components (such as windows and light shelves) as well [16]. For example, glass material has a major impact on user visual comfort [17]. On the other hand, energy optimization is also a significant part of investigation into offices with responsive facades and it showed a large reduction in energy consumption [18]. Considering energy efficiency in offices, new methods are also examined to improve building design process [19]. However, it is necessary to investigate a wider range of functions. For example, researchers have not pay enough attention to healthcare facilities, which play a major role in urban development programs and are built at various scales (small, medium, and large). Understanding the impact of hospitals on the environment and public health, the relationship between hospital buildings and the occupant's well-being is one of the major concerns in recent years. In healthcare buildings, in addition to diagnostic and medical activities, the basic approach is to provide a sense of calmness and comfort for patients, clients, and staff [20]. A hospital that is designed, built, and operated according to occupant demands, as well as existing standards, will lead to increased security, satisfaction, income, and comfort for all patients. Building design is greatly influenced by the occupant satisfaction in the indoor spaces, and many factors need to be considered at the time of design and renovation [21]. For instance, hospital users have several perspectives about their physical environment, including control, privacy and comfort [22].
Daylighting is a controllable factor, contributes to creating high-quality interiors, especially in healing environment. In these facilities, adequate daylight is directly related to diagnostics and treatments, and reduces the length of stay [23,24]. In various clinical studies, the effect of daylighting on different cases, such as drug consumption [25], suicides [26], mental disorders [27], sleep disorders [28-30], heart attacks [31], and stress [32] have been studied. Aside from examining the patients' condition, it is also necessary to consider the effect of the daylight on the staff comfort. Because the hospital staff spends many hours in various spaces under different conditions, that may affect their wellbeing [33].In general, excessive daylighting is not acceptable, and it should be limited to prevent overheating and glare [11]. Glare control is essential in medical spaces, especially a patient room, where the patient's comfort is the priority.
While numerous studies investigated daylighting indicators through the simulation and field measurement of some functions such as offices, an investigation into other uses like healthcare facilities is demanding. Consequently, as mentioned earlier, daylighting in healthcare spaces can be extremely beneficial and needs special consideration. Therefore, this study assesses patients' visual comfort in a hospital patient room with four different responsive facades and determines related factors.
2. Literature
Responsive facades are a practical solution to climate-based building development during recent years. In addition to adapting to the environment, they can reduce building energy consumption, adjust natural ventilation and daylight, and improve human visual and thermal comfort [34]. However, in terms of daylighting, there are some main factors that should be considered during their investigation process. Table 1 provides some beneficial information about this.
Table 1
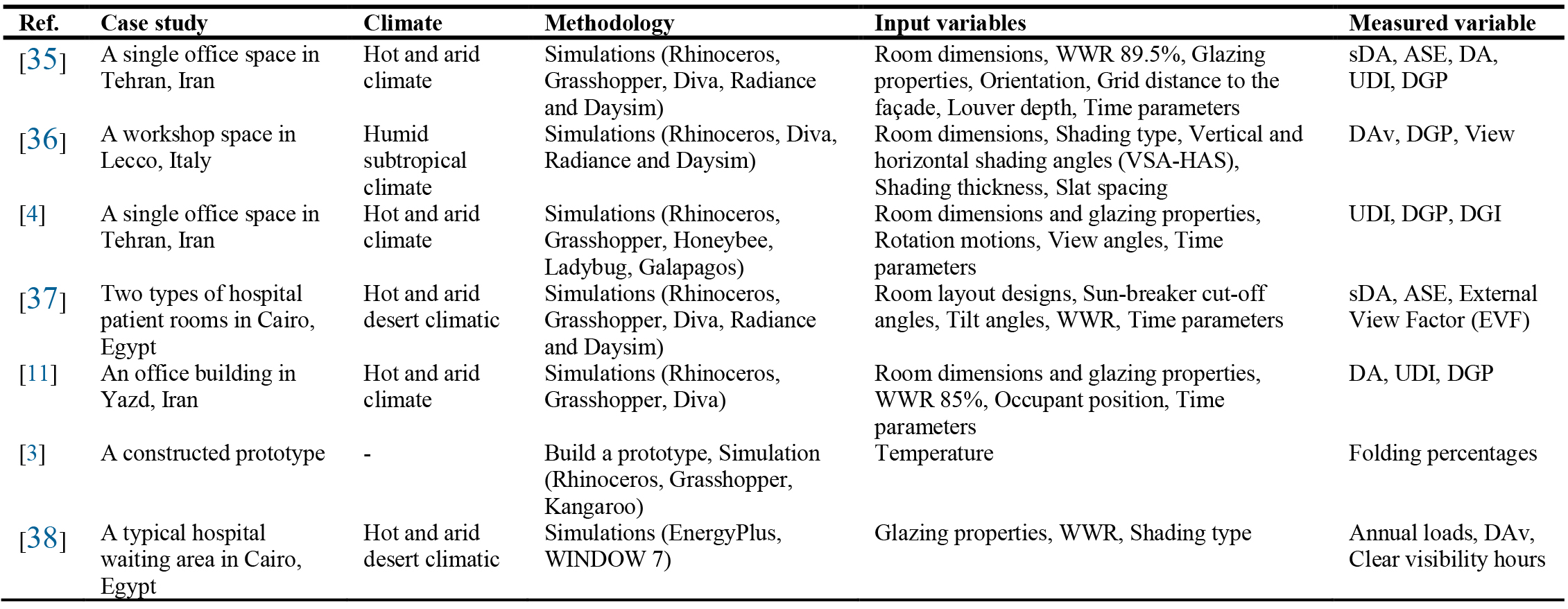
Table 1. Responsive facade literature details.
In terms of daylighting assessments in healthcare facilities, many studies have been conducted. The need for the existence of policies related to urban planning was felt from the middle of the 19th century, right at the time when a number of diseases became pandemic in many industrial cities. Improper natural ventilation and daylighting in the buildings overshadowed the treatment conditions and length of the patient stay [39]. Meanwhile, several studies have investigated the health benefits of daylighting., some of which have been mentioned below.
Alzoubi et al. [40] investigated Daylight Factor (DF) in the hospital patient room without considering the facade type. This study has a comparative approach between the simulation of the optimal state and the existing state. In the latter, the internal illuminance levels are higher due to the higher reflection of the internal surfaces. The results showed that, interior design parameters, such as furniture and indoor surfaces, have a direct relationship to indoor daylight quality. In another study by Choi et al. [41] the effect of interior daylighting on the Average Length Of Stay (ALOS) in the hospital wards was investigated. Moreover, the findings were compared based on two states of the visual discomfort caused by daylight reflection from the wall facing the patient and that by direct sunlight entering. It showed southern rooms gain more daylight than the others, while ALOS is more for north rooms. Morning illuminance also is more beneficial than daylight in afternoon. Alzoubi & Al-Rqaibat [20] have evaluated the indoor daylight quality of the children’s section of King Abdullah hospital by field measurements and simulations. In the south and north patient rooms, illuminance and luminance levels were higher than CIBSE standards, meaning the hospital facade needed to be shaded.
One of the factors affecting indoor illumination is glazing, which has been less discussed in the studies related to hospitals and daylighting. Sherif et al. [42] have compared Daylight Availability (DAv) of three different room layouts and three different glazing types (Electrochromic-30, Electrochromic-60 and double pane Low-E-Argon-filled glass) with various WWRs. The study found that when the bed is far from the window with Electrochromic-30 glazing, it did not have an acceptable result in any WWR. Also, when the bed is close to the window, Low-E and Electrochromic-60 glazing types create over-lit and inappropriate conditions. It is important, however, to consider the climate at the time of choosing glazing types for installation. For example, shading and proper glazing type for wider windows can reduce cooling energy consumption in hot climate [43]. Sherif et al. [44] also carried out another study focusing on the shape of the slats of the indoor blinds in the patient's room and its effect on daylighting. In this research, the external view factor is also evaluated in two different patient positions, lying and lateral recumbent. A geometric shape that has been optimized is then presented. As a weakness, the study lacks the user's involvement in adjusting shading and external view, and the illumination level, which according to the writer's perspective, can be problematic in some cases. Englezou & Michael [45] evaluated various factors, including ASE for 15 different WWRs for single and double patient rooms. In addition, sun chart was used to calculate the horizontal louver width and determine its role in indoor daylighting. Simulation results were also compared with on-site measurements. It was found that both rooms perform well according to the Useful Daylight Illuminance (UDI). But in smaller room, when the window is large, there is a high probability of glare. According to the results, several parameters must be studied simultaneously to choose the best condition of daylighting from all aspects. Al-Shafaey et al. [46] have focused on the number and depth of horizontal louvers on double-skin facades and investigated the visual comfort factors in a patient room in Cairo, Egypt. In addition to finding the best option, the results have shown that the facade performance by any kind of louver will be better than the facade without protection. Wagdy et al. [37] also evaluated the angle of horizontal louvers for two types of hospital rooms and different WWRs. They concluded that by increasing WWR, the number of comfortable conditions also increases. The acceptable results of spatial Daylight Autonomy (sDA) in the inboard room layout are more than the outboard one. Furthermore, artificial lighting is used in hospital rooms in addition to daylighting during certain times of the day and night. Therefore, it is necessary to control the electrical energy consumption and choose appropriate lighting sources [47]. Artificial lighting has a considerable impact on the productivity and accuracy of medical processes [48].
In the healing environment, in addition to considering the patient room, it is also important to consider the public spaces (e.g. the lobby), as well as the staff areas. Accordingly, a study has been conducted on how hospital staff prefer to view nature-based content from their break areas, in order to reduce their stress and restore energy [49]. The method was through an online survey, including 50 questions in six parts. These six sections include general information such as age, education, job title, and work experience. For the main part of the survey, simulated images of five different break areas were used. According to the results, staff prefers rest areas with access to the outside environment (terrace and balcony). However, the findings are for a specific climate and can be different in other climates conditions. Sun & Huang [50] have investigated the energy and daylighting of different layouts of five hospital lobbies with different locations. Following that, in two stages, considering the design of the space (location-orientation-height) and the design of the facade (WWR - Skylight ratio), various options were compared. Based on the results, height impacts energy consumption more than its location and orientation, but it has no significant effect on daylight. It is also more effective to change the skylight ratio than to change the window size on the average daylighting. Sadek & Mehrous [38] also investigated using adaptive glasses in a hospital waiting area in Egypt. In addition, three different types of shading (vertical, horizontal, and perforated screen) were evaluated. A horizontal shade provided a transparent window and an outside view for longer hours, according to the results. Also, the horizontal shade showed the best performance in energy saving compared to the vertical shade and perforated shade.
Clearly, there has been less research on responsive facades, particularly with parametric patterns, except for conventional designs (horizontal louvers and simple shades), in hospital buildings. Therefore, to fill the identified gaps, this study evaluates the visual comfort of patients in a typical patient room of hospitals with four different responsive facades and investigates related indicators. Moreover, results are validated through Leadership in Energy and Environmental Design (LEED v4) certification and software validation.
3. Materials and methods
This study is classified as applied research and offers suggestions to provide visual comfort using responsive facades in hospitals. As the first step, based on previous studies and collected information, a sample of a main area of the hospital, a typical patient room, is modeled as a baseline model for simulation. Moreover, four various responsive facades are selected for planed investigations under different conditions through simulation. The baseline model, static façade, and responsive façade are first compared based on the solar access index. Following that, annual sunlight indicators are assessed for all cases to consider their long-term function. At the end, with a quantitative approach, the simulation outputs are compared to select the optimal facade model. To achieve this, glare indices are simulated for optimal WWR and façade so that the facade is examined in more detail. A research flowchart is also provided to clarify an overview (Fig. 1).
Figure 1
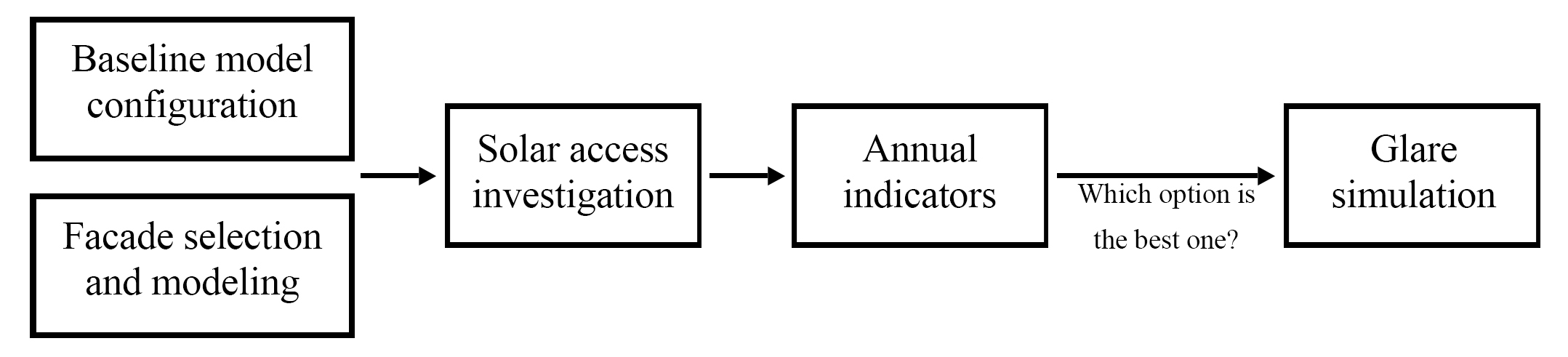
Fig. 1. Research flowchart.
Parametric design tools were presented and used as new options since 2008 by several software development companies, such as Catia, 3Ds Max, Maya, Revit, Dynamo, and Grasshopper. However, one of the most common tools is Grasshopper [51]. This parametric tool has been used in this study by using some widely used plugins for daylighting and climate, including Honeybee and Ladybug [52], which has been validated before [53,54]. Honeybee creates and visualizes the results of daylight using Radiance engine, uses backward ray-tracing method. Since the research studies climate-based metrics, the weather condition is taken from online data base of EnergyPlus [55].
Calculated annual metrics include sDA and ASE. The former shows the percentage of the floor area that receives minimum of 300 lux for at least 50% of the annual occupied hours, while Annual Sunlight Exposure presents the percentage of the floor area that receives at least 1000 lux for minimum 250 hours per year [56]. Moreover, investigated daylight glare indices are Daylight Glare Index (DGI) and Daylight Glare Probability (DGP), both are introduced in several studies [57].
3.1. Selected city
Tehran (35.7 Latitude and 51.4 Longitude) is the capital of Iran. It is classified as a hot semi-arid climate (BSh) in the Köppen classification system. Tehran's northern part has moderate weather because of the Alborz Mountain range, and in the southern areas, it is semi-arid. The relative humidity is also low. To provide comfortable conditions, it will be efficient to use passive strategies. The visual output of the annual total, diffuse and direct sun radiation in Tehran is provided (Fig. 2)
Figure 2
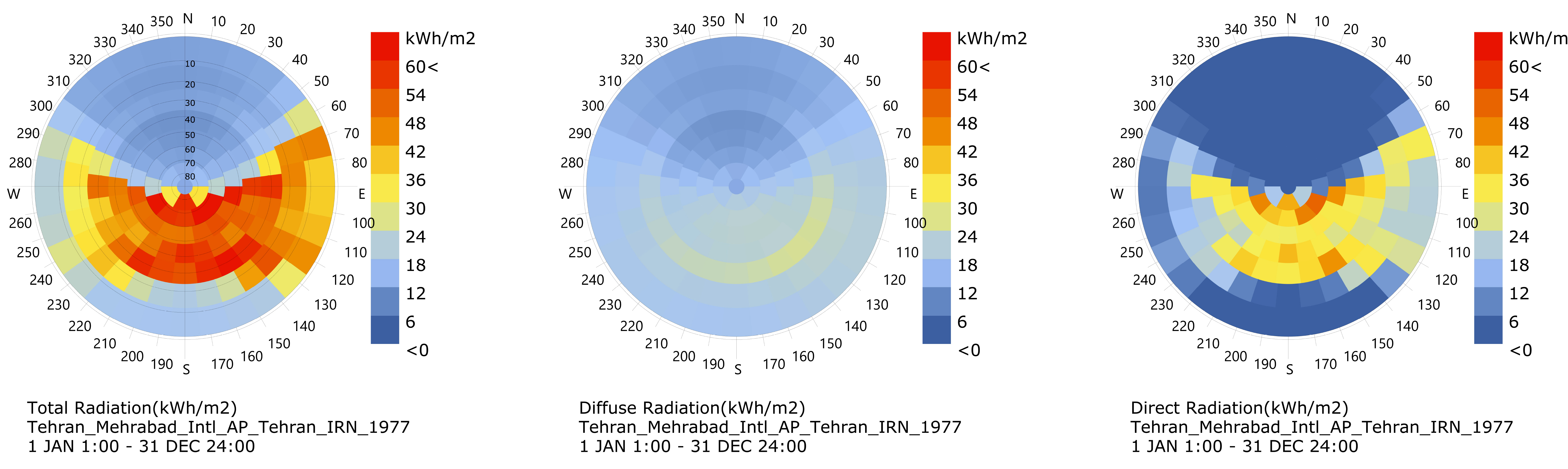
Fig. 2. From left to right: annual total, diffuse, and direct sun radiation in Tehran.
3.2. Simulated model
In order to investigate the daylighting conditions in healing environment, a standard model of a south faced two-bed patient room measuring 4.2 meters wide, 7.5 meters long, and 3.5 meters high, and with an area of 31 square meters, was modeled in Rhinoceros. The room has a window that will have variable WWRs (Fig. 3). This room is considered the baseline model throughout the study.
Figure 3
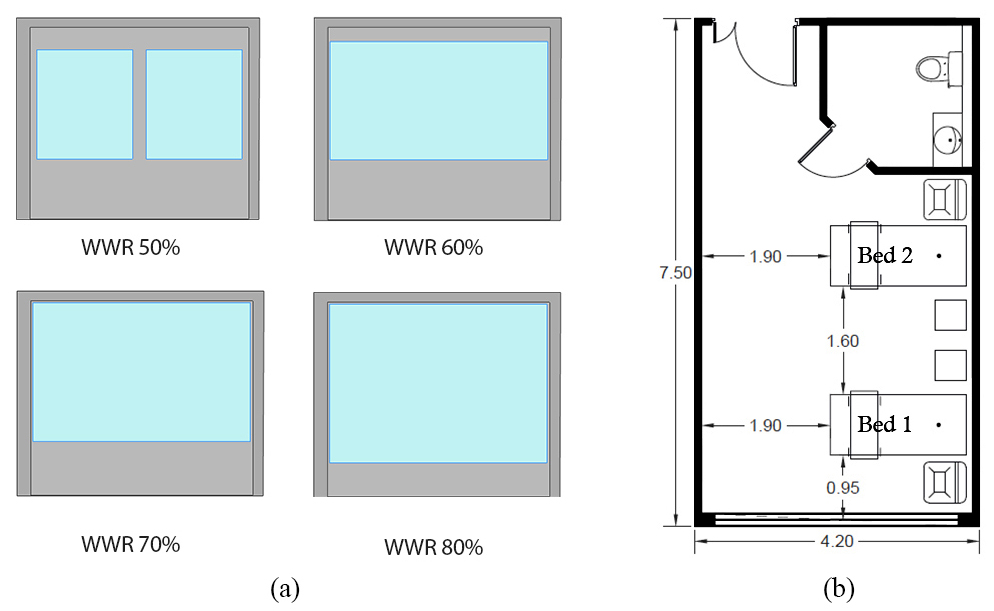
Fig. 3. (a) Examined window to wall ratio and (b) Baseline patient room model dimensions.
The bed, which is closer to window, is considered bed one and the other one is considered bed two. Another highly influential parameter in indoor daylighting is the reflectance of the indoor surfaces, which are recommended by LEEDv4, for building design and construction, [58] and has been used in several similar articles [37,42,44] are described in Table 2.
Table 2

Table 2. Responsive facade literature details.
The simulation grid height was set at 90 centimeter above the floor at the level of the patient's bed. In addition, to have a high accuracy of the grid-based simulation, the dimensions of the network were defined as 10 x 10 centimeter. Moreover, to measure the amount of glare, which is dependent on the location of the observer, the position of the patient's head has been introduced to the plugin as the critical point. Radiance engine parameters, which have been proposed by software, are listed in Table 3.
Table 3

Table 3. Radiance engine parameters.
3.3. Responsive façade models
Four moving facades were algorithmically coded in Grasshopper, and the sun location was introduced as an attraction point to the facade elements. Patterns are selected for facades in such a way that they are used in existing buildings (Al-Bahar tower and Kiefer technical showroom) or are similar to conventional patterns. Furthermore, facade movement is considered to be in different axes. Therefore, façade one and two have diagonal, façade three has horizontal and façade four has vertical axes. These movements are done in two ways: folding and basic rotation. Each façade has its own grid based on the geometry. For example, in façade 1 and 2 front surface is divided into four sections by width and length and each section measures 105 x 87 centimeter. The third facade has a 3x10 grid and the fourth one has a 2x8 grid. Thus, the former panel is 42 x 115 and the latter is 52 x 175 centimeter. Figure 4 shows the various states of each facade at its most open and closed state and at three different times of day when WWR is 70%.
Figure 4
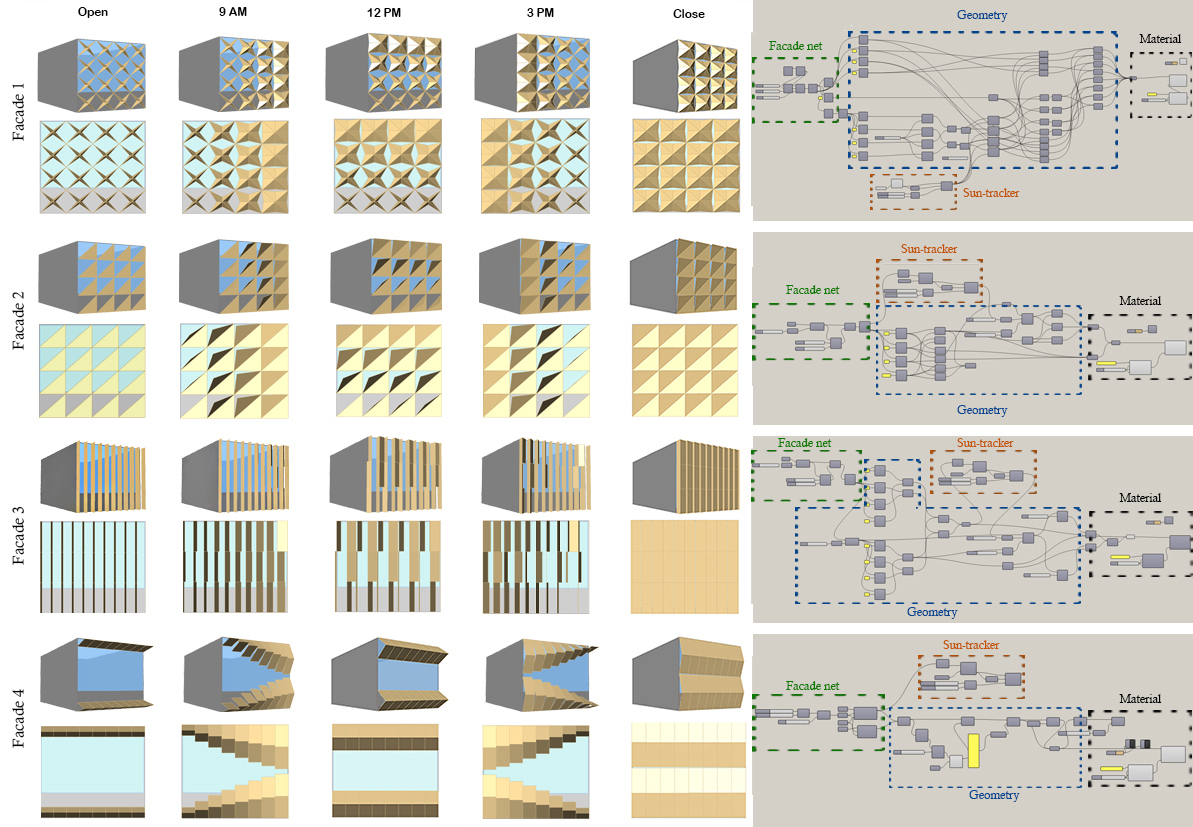
Fig. 4. Simulated facades.
4. Findings
4.1. Solar access
As the first step, direct sunlight has been measured in the patient room to determine the impact of the responsive facade. Accordingly, the simulated maps are as follows at 12 pm on December 21st and with the largest WWR (80%) where the amount of sunlight is maximum. In addition to the responsive mode, the static mode of the same facade has also been evaluated. It is apparent from the results (Fig. 5) that a responsive facade will allow for better control over solar access. Since solar access is 62% for baseline model, yet for all other responsive facades it is less than 30%. Façade one and four have the less percentage with 18% and 16%, respectively.
Figure 5

Fig. 5. Solar access at 12 pm on December 21st.
4.2. Annual indicators
The healing places, like hospitals, are active 24/7 throughout the year. In addition, the patient room is a function where the user may have to spend a long time, as long as several weeks. Thus, long-term comfort should be provided and annual indicators need to be checked. As a part of this step, annual indicators, including spatial Daylight Autonomy (sDA), and Annual Sunlight Exposure (ASE) are investigated (Table 4).
Table 4

Table 4. Radiance engine parameters.
As proposed by LEEDv4 certificate, ASE should not exceed 10%, and sDA should be at least 55% in normal conditions and 75% in healthcare facilities. Considering upper mentioned results, façade two and façade four cannot meet the proposed values of ASE, but it is approved by WWR 50% and 60% for the façade one, and by WWR 50% for the façade three. Although sDA has passed the minimum requirements in all cases, ASE acts as a limitation. As a result, facade one has a better performance compare to other facades, while Facade 4 has the worst performance.
4.3. Glare
In a treatment environment, especially the patient room, where one should not expect unnecessary movement and activity to eliminate annoying factors, controlling glare requires more attention. Inevitably, glare irritates the eyes, reduces vision, and sometimes causes health problems such as headaches and dry eyes. In addition, this index is one of the most important indicators for measuring visual comfort. It occurs when the window is placed in an inappropriate orientation, has incorrect dimensions, and the shade is not used in the proper position or at the correct time.
In order to determine glare, on December 21st, the shortest critical day of the year, when the sun is at its lowest position, visual comfort conditions can be evaluated. Therefore, the outputs of DGP and DGI indicators have been calculated for the three hours (9, 12, 15) and the position of patient head in both beds during rest.
In order to compare two beds according to the results of Tables 5-9, Fig. 6 is helpful. As it is clear from the results, in all cases, at 9 o'clock, there are only slight differences between the baseline model and four other facades. Furthermore, at 12 o'clock, the patient in the first bed (close to the window) will suffer from glare. Although by using the first and third facades, there will be no problem for the bed one patient in the morning and afternoon, the second and fourth facades cause glare in the afternoon. Due to the position of the patient's head, this problem can appear symmetrically in the adjacent room in the morning. On the other hand, the patient in the bed two with the first facade did not experience glare during the three hours of observation. While at 15 o'clock three other facades cause unpleasant conditions. Façade three also results in the worst performance for the same patient. Therefore, regarding the first bed, the worst performance is for facade 4 and the best is for facade 1. Although facade 3 performs well in the first bed, for the second bed, it has performed inappropriately due to the verticality of the facade structure, which leads to disproportionate penetration and reflection of sunlight. Renders of glare outputs for two different WWRs (50% and 80%) and two beds are presented in Fig. 7.
Table 5
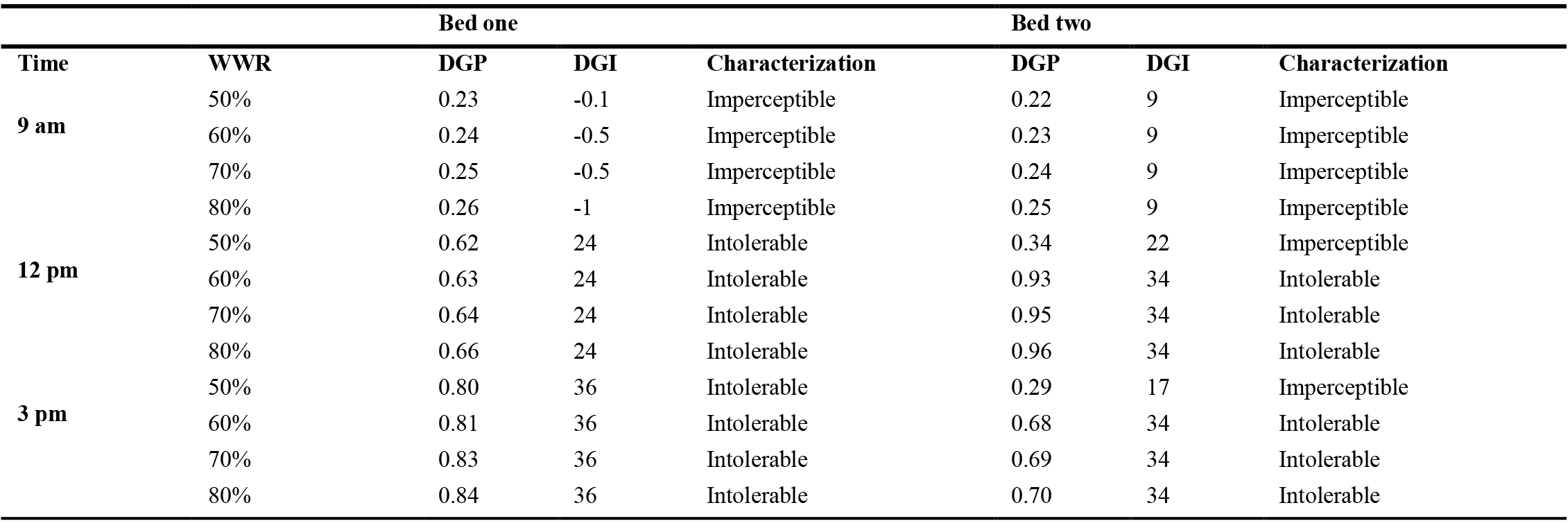
Table 5. Glare for the baseline patient room without responsive façade.
Table 6
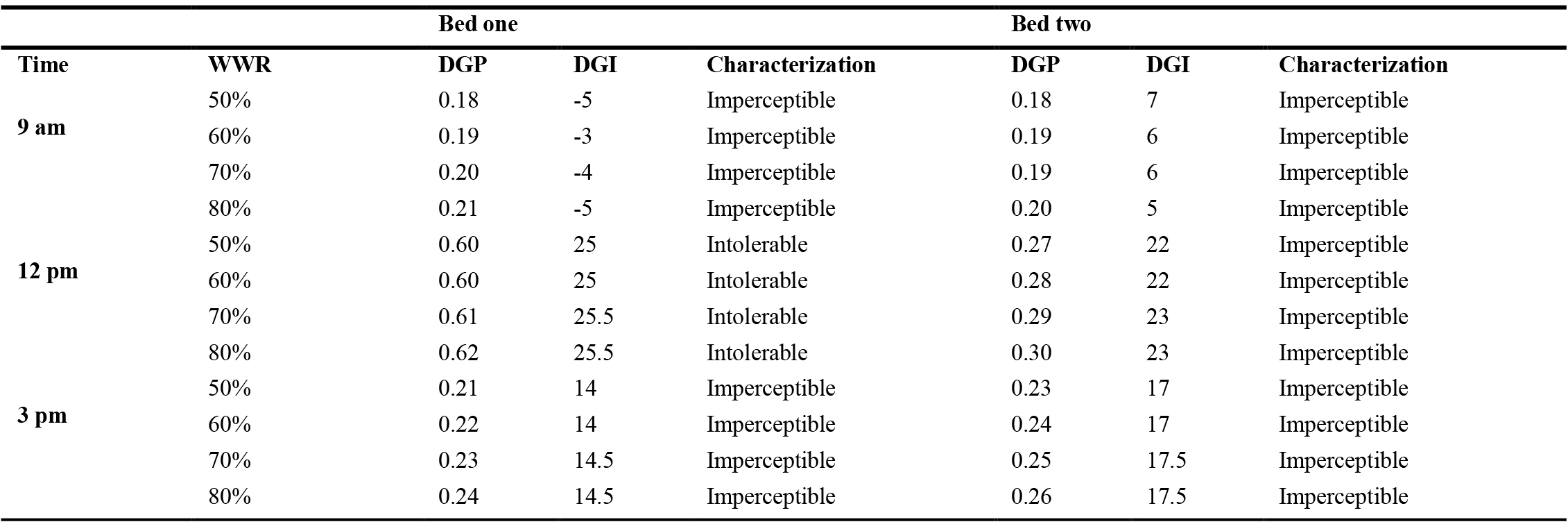
Table 6. Glare for the patient room with facade one.
Table 7
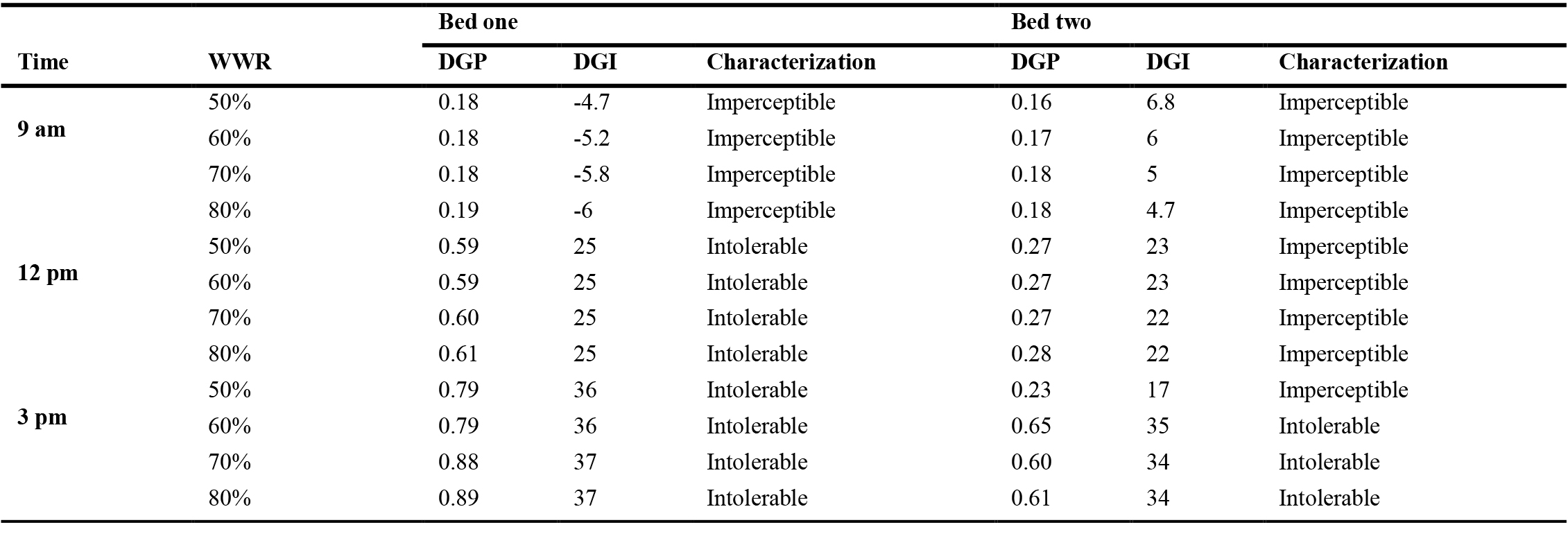
Table 7. Glare for the patient room with facade two.
Table 8
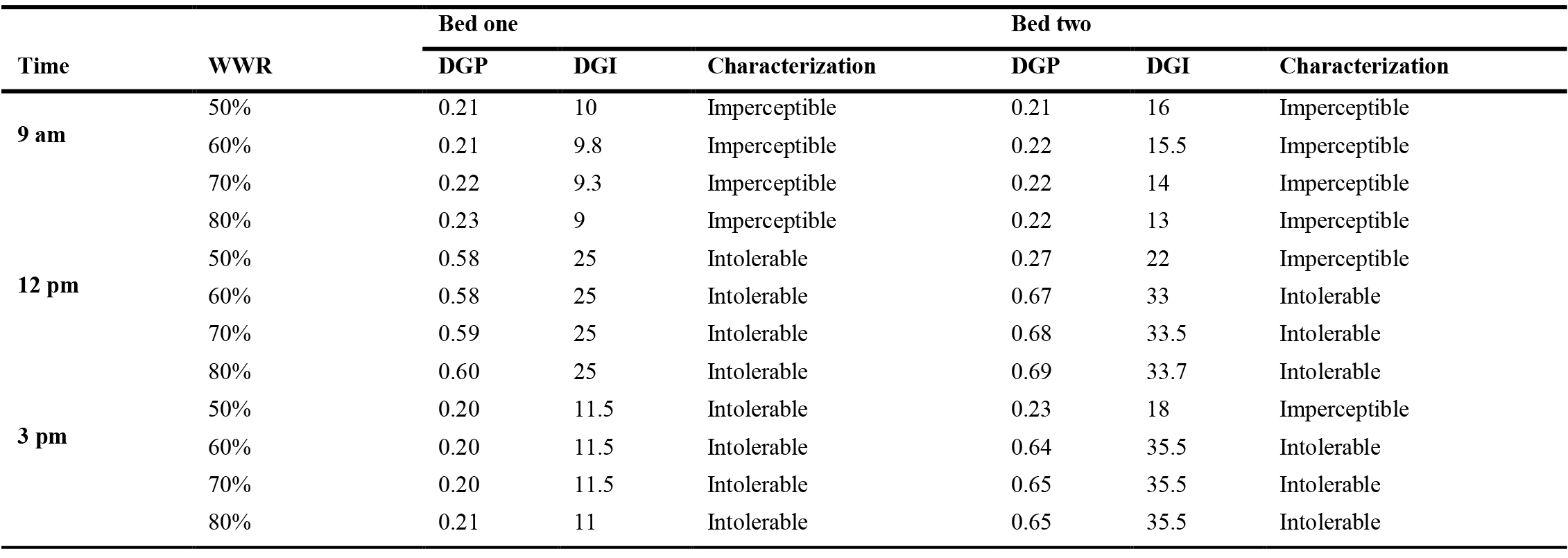
Table 8. Glare for the patient room with facade three.
Table 9
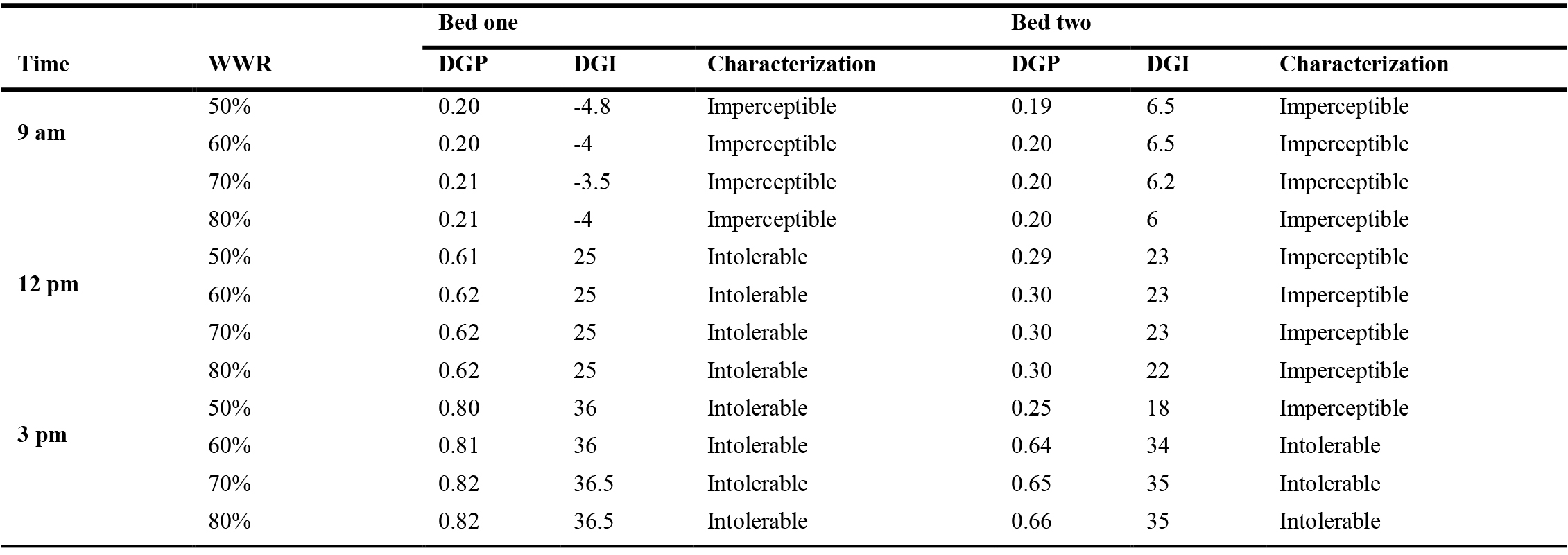
Table 9. Glare for the patient room with facade two.
Figure 6
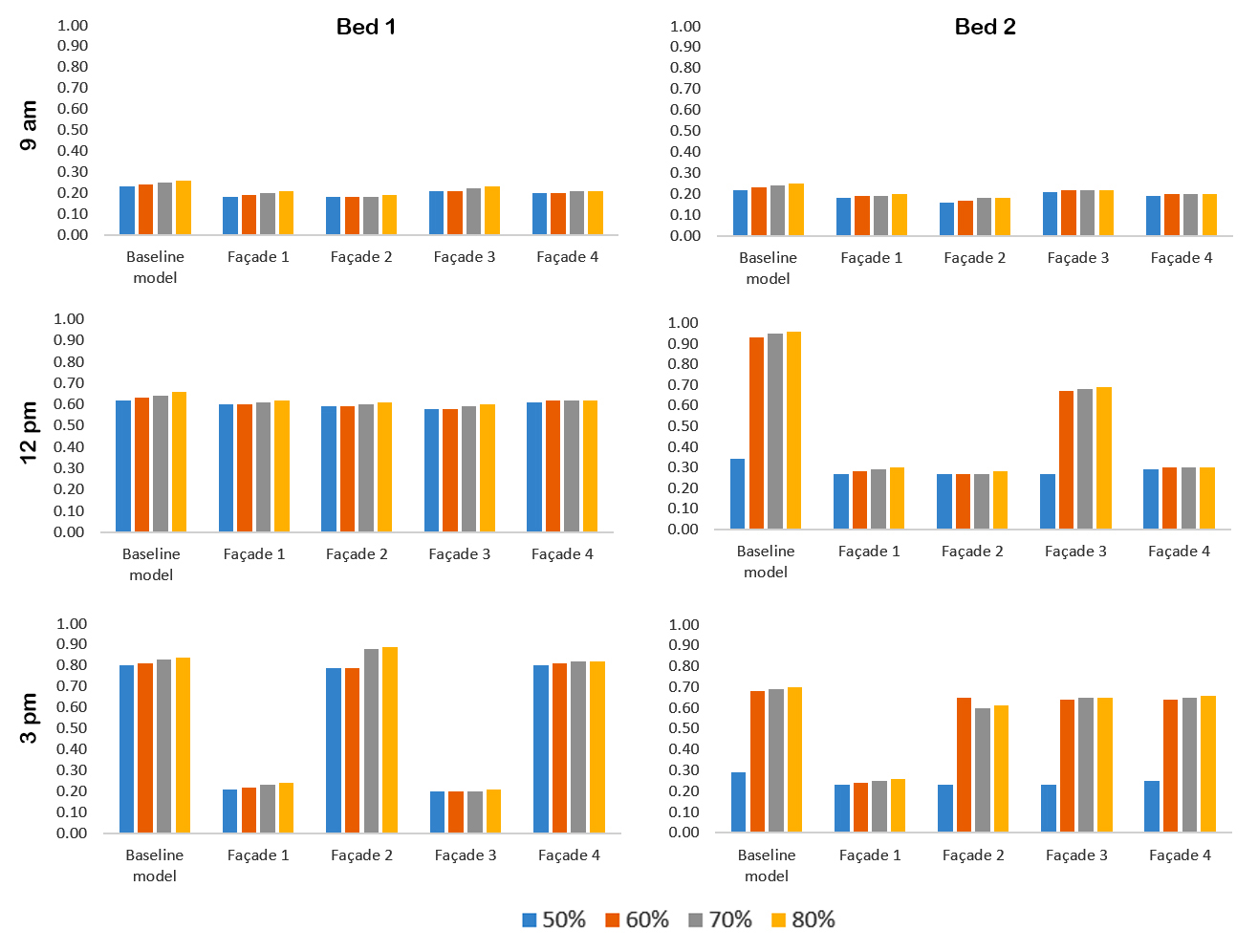
Fig. 6. Comparison of DGP for bed one and bed two in all cases.
According to the results of the solar access, annual indicators and the glare, facade one is considered to perform better compare to three other facades. In the following, DGP is calculated for one day per month in all daylit hours and for both beds to check the possibility of glare more precisely in the selected facade. According to ASE reports and LEEDv4 guidelines, acceptable WWRs for facade 1 are 50% and 60%. Considering that sDA with a larger window is more desirable, 60% was selected for further investigation.
Figure 7
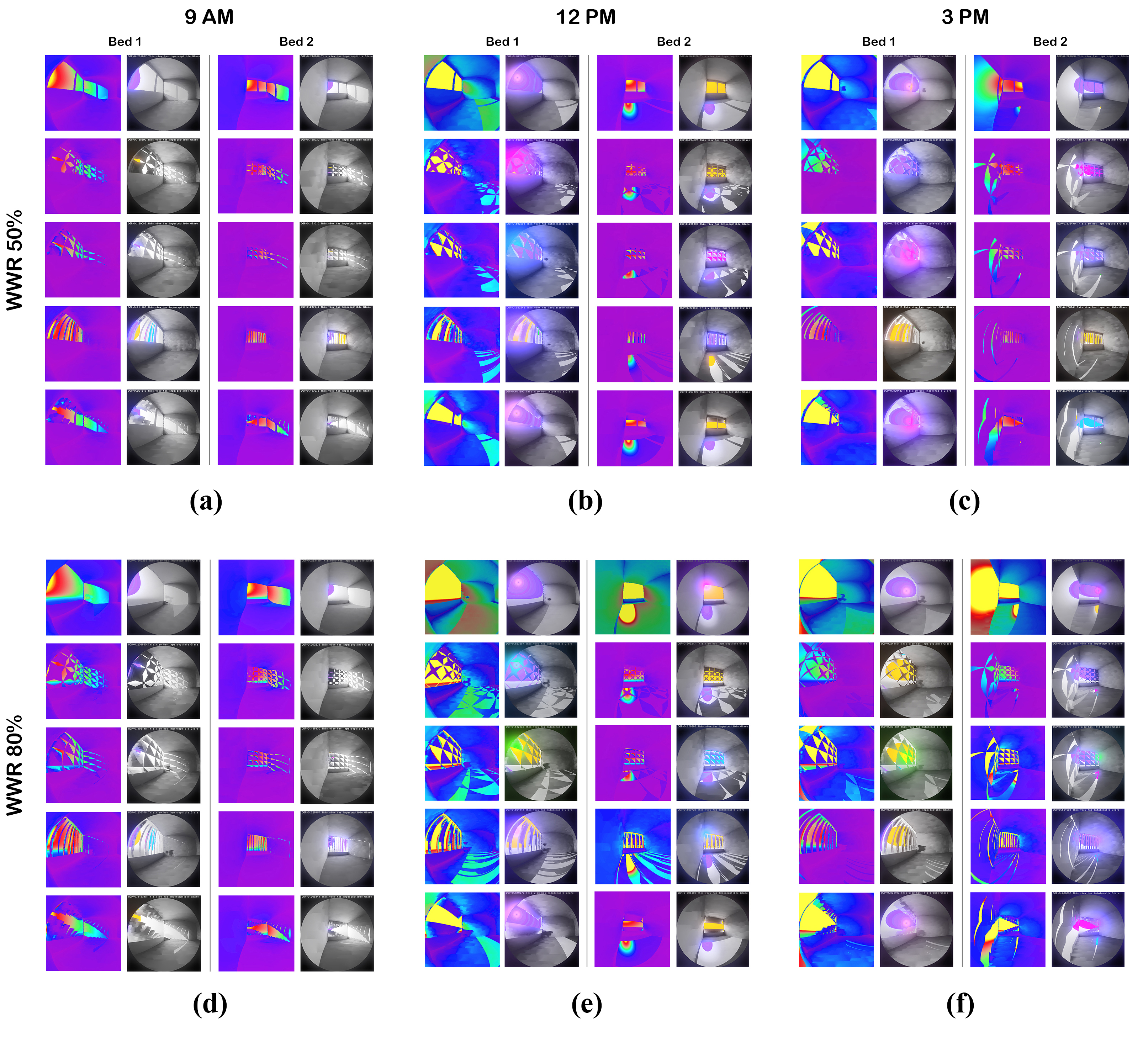
Fig. 7. False color and renders of glare outputs for (a) WWR 50%, 9 am (b) WWR 50%, 12 pm (c) WWR 50%, 3 pm (d) WWR 80%, 9 am (e) WWR 80%, 12 pm (f) WWR 80%, 3 pm.
Firstly, all hourly outputs were measured for the baseline model which is a room without a responsive façade (Table 10). The results show that from October to April, in the hours before noon to the afternoon, the patient in bed one witnesses glare. Furthermore, the results of bed two show DGP of more than 0.35 from November to March between 11:00 and 17:00.
Table 10
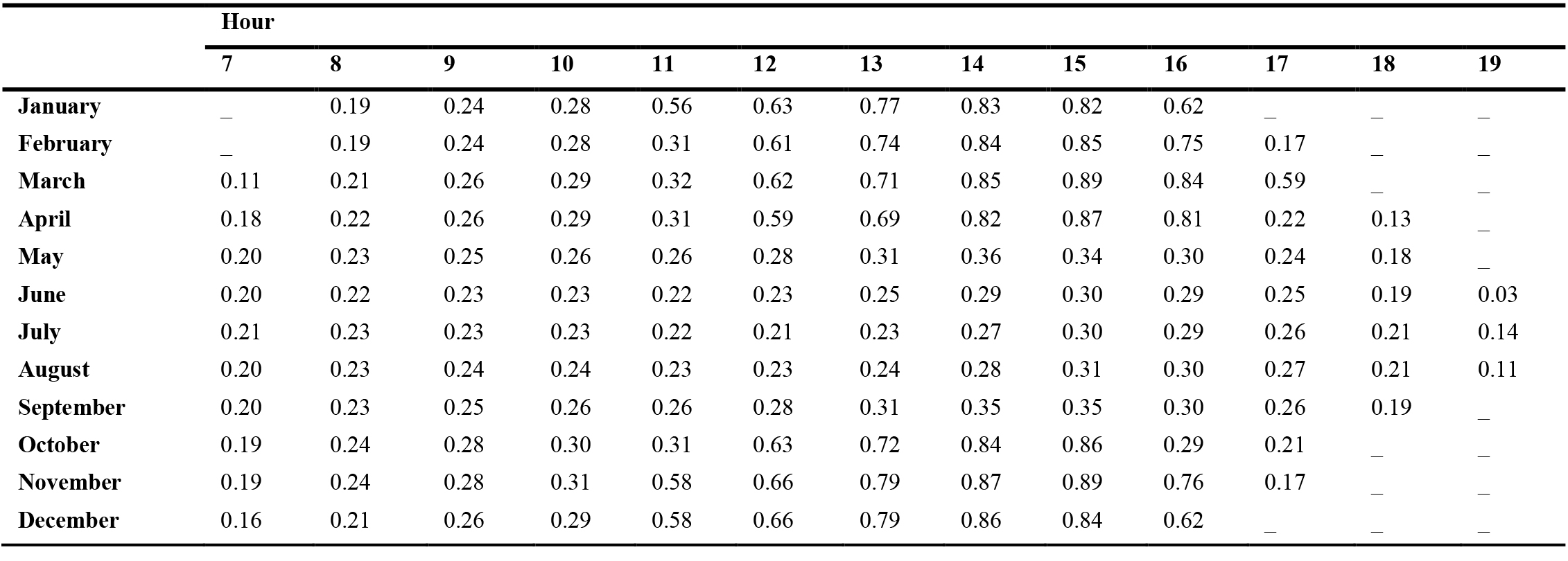
Table 10. Hourly DGP for different month and for baseline model of patient room which is without responsive facade (WWR:60% - Bed one).
Then, to measure the effectiveness of the responsive facade in similar conditions, the hourly data of the hospital patient room with facade one is calculated for both beds (Tables 11 and 12).
Table 11
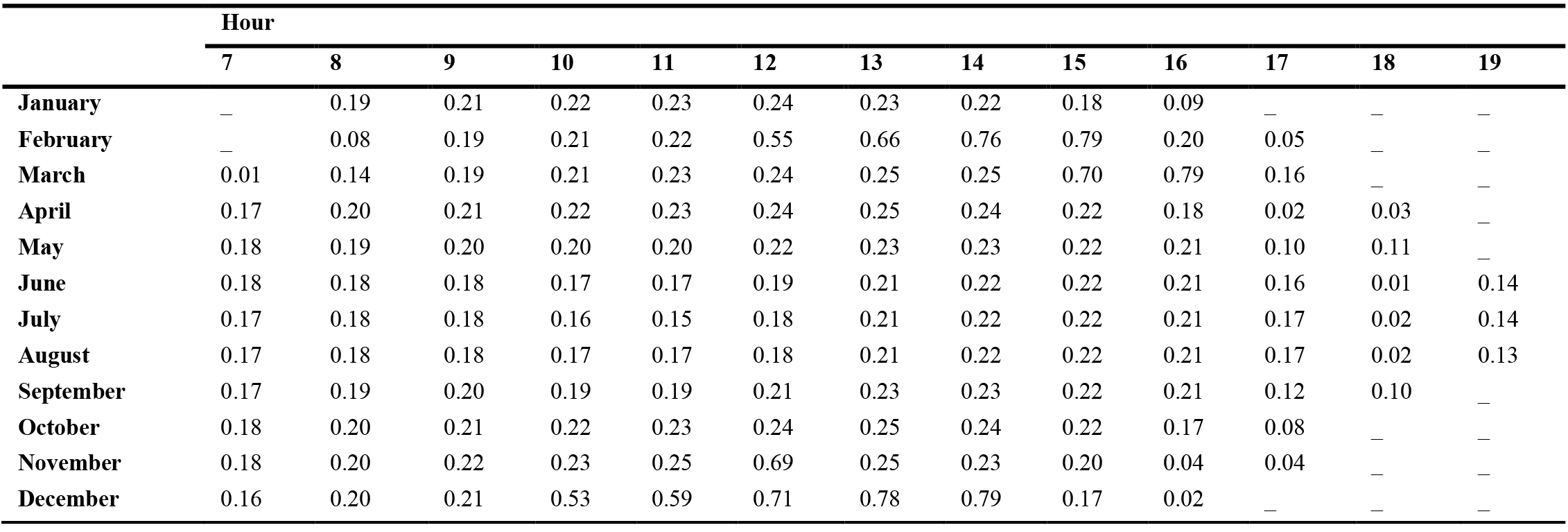
Table 11. Hourly DGP for different month and for patient room with facade one (WWR: 60% - Bed one).
Table 12
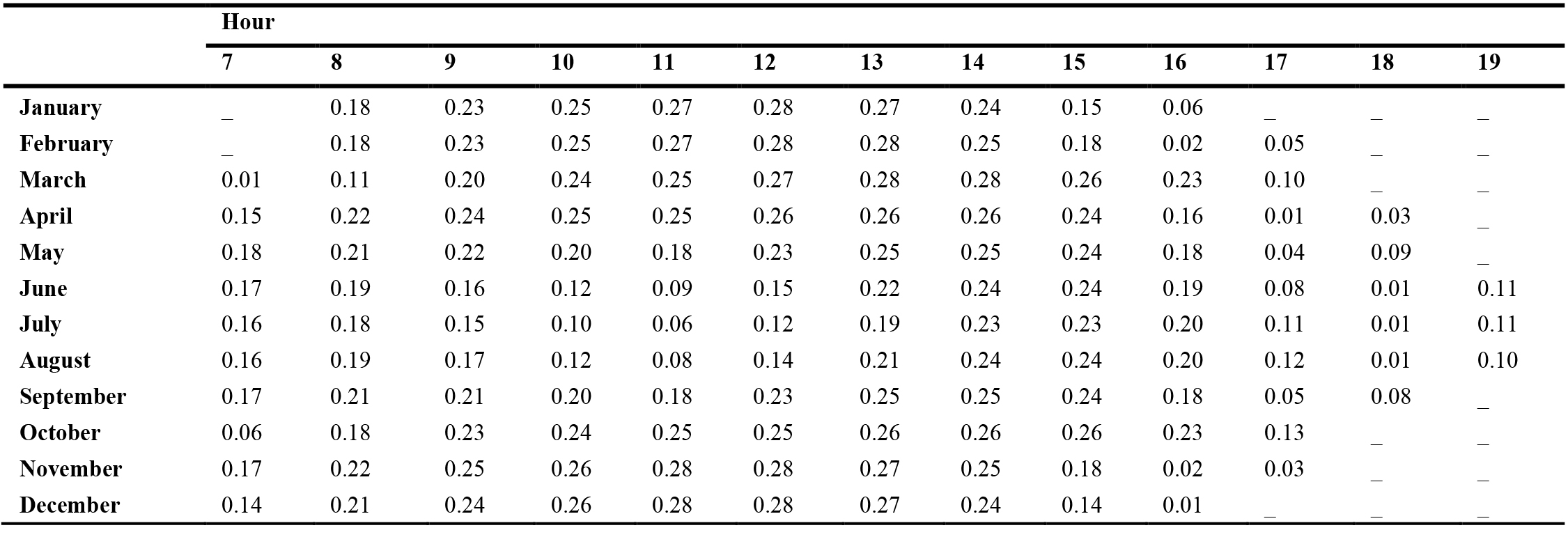
Table 12. Hourly DGP for different month and for patient room with facade one (WWR: 60% - Bed two).
As the results have shown, glare for bed one has been largely eliminated. It only occurs at 12 pm in November, some hours in December and February, and at 15 and 16 in the afternoon in March. Regarding bed two, by applying the facade, the glare is completely resolved, and a proper comfort condition is provided for the patient.
5. Discussion
Four selected facades have been investigated through some stages. Firstly, solar access is examined for baseline model, static façades and responsive facades. Results showed that façade one and façade four have the best performance and they received 71% and 74% less direct sunlight compare to baseline model, respectively. Following that, ASE and sDA are investigated for all cases and results revealed that façade two and façade four cannot meet the limitations of LEEDv4 certification. On the other hand, façade one (WWR 50% and 60%) and façade three (WWR 50%) showed acceptable values. For example, ASE improved around 81% for façade one WWR 60% and just above 77% for façade three WWR 60%. Since glare is an essential part of visual comfort, more investigations have done considering DGP and DGI for four façades for three specific hours and both beds. As it was obvious, results were totally different for bed one and bed two. However, façade one showed the best performance. Considering 3 pm, this façade performed 75% better for bed one and 65% better for bed two compare to baseline model. Furthermore, in 12 pm, façade one improved glare condition just above 68% compare to baseline model. According to the findings of all the stages of this study, façade one can be considered the ideal choice among the examined options. However, as the results of this facade showed, in some hours of the year, the patient will still suffer in the bed. Therefore, it is necessary to check if using a smaller window solves the problem or not. The other acceptable option in terms of annual indicators is a smaller window (WWR 50%), which despite the lower ASE, less useful daylight will enter the room.
The results showed that the smaller window has no effect on the glare for the first bed and the values of this index are almost the same as before (Table 13). Yet for the second bed, even without any facade, glare is imperceptible, and only in November, we will have perceptible glare during mid-day (Table 14).
Table 13
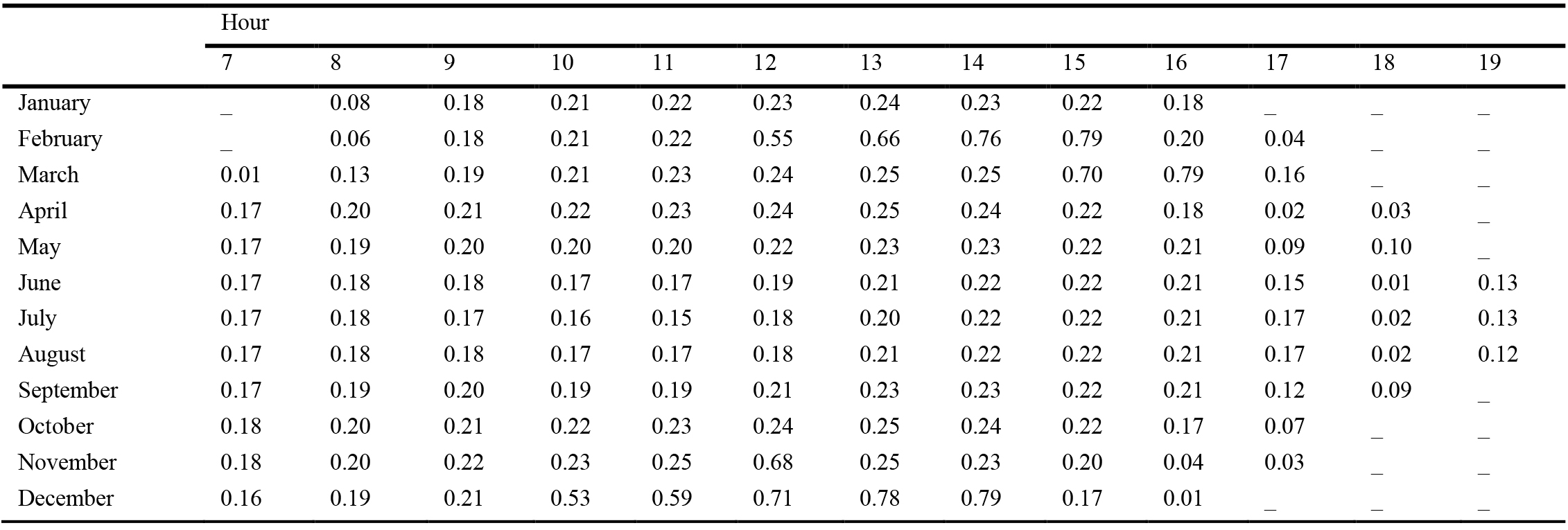
Table 13. Hourly DGP for different month and for patient room with facade one (WWR: 50% - Bed one).
Table 14
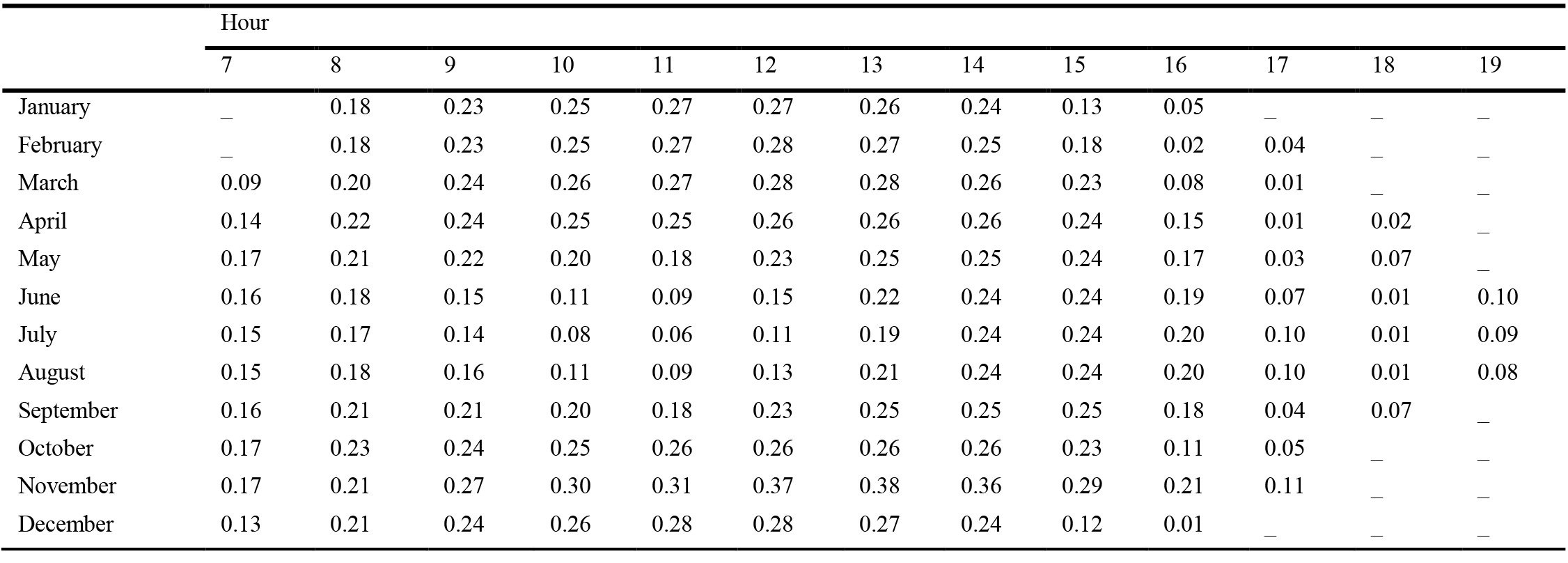
Table 14. Hourly DGP for different month and for patient room with facade one (WWR: 50% - Bed two).
These results indicate that the distance between bed and window has a direct effect on glare. By the correct placement of the indoor furniture, increasing the length of the room, changing the layout (as it is investigated in another research [37]), and if possible, turning the double-bed room into one-bed, the glare in a room with a WWR 50% and without a responsive façade could be controlled. If it is not likely to create a larger room or the user density in the treatment complex is high, it becomes necessary to use a protective element in the facade, such as the responsive facade. Otherwise, the patient in bed one or close to the window will suffer from glare during some hours of the year. In addition, by using a window with larger dimensions and not using a protective element, such as a curtain, glare will occur for both patients. Larger windows are also defined as a cause of glare in other studies [45]. Therefore, as results showed, using a protective element have many beneficial points compared to unprotected windows, as in other studies [44,46] has been stated. Although application of these responsive façades could result in limitation of patient view, there is some evidences that show higher positive effect of daylight on patients [59,60].
6. Conclusions
Increasing the comfort of users in indoor spaces has always been one of the concerns of designers and researchers. One of the main factors of creating indoor visual comfort is the presence of quality daylight. When it comes to boosting the quality of the built environment and the health of communities, one of the important functions that plays an essential role is hospital. It is beneficial to move the building towards the use of new technologies in order to achieve the desired goals in the design. In this study, the possibility of using one of these technologies, responsive facades, has been investigated in a therapeutic building to determine how effective such facades are in providing comfort. For this purpose, a typical patient room in Tehran was selected to investigate different daylight factors by simulation tools. Four different responsive facades were also compared under the same conditions. From the comparison of annual indicators including ASE and sDA, and the results of glare indexes including DGP and DGI, it was determined that the best and the worst performance is for façade one and façade four, respectively. By summarizing all outputs, the following results are obtained:
- When a fundamental issue, such as visual comfort, is being assessed in an important place such as hospital, considering one factor and measuring only one index is not enough to reach a conclusion, and different aspects should be considered.
- Using responsive facade does not only lead to better daylighting conditions and can also bring undesirable results. For example, the reflection caused by facade panels or shading may create glare and disturbs the comfort of the occupant.
- The window size has no effect on the glare of the person who is closed to the window, but in case of further distances, patient will not be glared without the presence of responsive facade. Therefore, if more daylight is demanded, the number of people in the room should be reduced or its area should be increased to provide the desired distance of bed from the window. Moreover, alteration in rooms layouts can be considered as a practical solution. Otherwise, there will definitely be a need for shading, light shelves and smart facades.
- Although in this study, WWR does not have a significant effect on glare, it will still be effective in daylighting and other related factors such as sDA and UDI. Considering façade one, ASE and sDA are acceptable when WWR is 50% and 60%, yet the larger one provides higher sDA.
- Among four examined facades, façade one which has diagonal movements in various axes has the best performance. Conversely, façade four which has vertical movements and its shading panels are less flexible is less efficient. Therefore, the more flexible the façade is, the more efficient it will be.
- Using the chosen responsive facade will greatly help to provide visual comfort and reduce glare. But even in the best case, due to ASE assessment, the glare could occur in some distances and hours of the year. In this situation, it is suggested to provide a simple barrier such as an internal curtain to be used by the patient or other people in the room if needed. It is obvious that curtains with remote control are more convenient for patients.
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by H. Toodekharman. The first draft of the manuscript was written by H. Toodekharman and review and editing were done by M. Abravesh. S. Heidari and M. Abravesh were also supervisors. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of competing interest
The authors declare no conflict of interest.
References
- N. Stevulova, K. Baltakys, A. Estokova, V. Vaclavik, S. Dimter, Sustainable Building Materials and Technologies 2020, Advances in Materials Science and Engineering 2022 (2022) 9797342. https://doi.org/10.1155/2022/9797342
- M. Dabbagh, M. Krarti, Evaluation of the performance for a dynamic insulation system suitable for switchable building envelope, Energy and Buildings 222 (2020), 110025. https://doi.org/10.1016/j.enbuild.2020.110025
- M. Pesenti, G. Masera, F. Fiorito, M. Sauchelli, Kinetic Solar Skin: A Responsive Folding Technique, Energy Procedia 70 (2015) 661-672. https://doi.org/10.1016/j.egypro.2015.02.174
- A. Tabadkani, M. Valinejad Shoubi, F. Soflaei, S. Banihashemi, Integrated parametric design of adaptive facades for user's visual comfort, Automation in Construction 106 (2019) 102857. https://doi.org/10.1016/j.autcon.2019.102857
- SM. Hosseini, M. Mohammadi, A. Rosemann, T. Schröder, J. Lichtenberg, A morphological approach for kinetic façade design process to improve visual and thermal comfort: Review, Building and Environment 153 (2019) 186-204. https://doi.org/10.1016/j.buildenv.2019.02.040
- A. Ghosh, B. Norton, Advances in switchable and highly insulating autonomous (self-powered) glazing systems for adaptive low energy buildings, Renewable Energy 126 (2018) 1003-1031. https://doi.org/10.1016/j.renene.2018.04.038
- RCGM. Loonen, M. Trčka, D. Cóstola, JLM. Hensen, Climate adaptive building shells: State-of-the-art and future challenges, Renewable and Sustainable Energy Reviews 25 (2013) 483-493. https://doi.org/10.1016/j.rser.2013.04.016
- A. Tabadkani, A. Roetzel, HX. Li, A. Tsangrassoulis, Design approaches and typologies of adaptive facades: A review, Automation in Construction 121 (2021) 103450. https://doi.org/10.1016/j.autcon.2020.103450
- A. Eltaweel, Y. Su, Parametric design and daylighting: A literature review, Renewable and Sustainable Energy Reviews 73 (2017) 1086-1103. https://doi.org/10.1016/j.rser.2017.02.011
- S. Fattahi Tabasi, S. Banihashemi, Design and mechanism of building responsive skins: State-of-the-art and systematic analysis, Frontiers of Architectural Research 11(6) (2022) 1151-1176. https://doi.org/10.1016/j.foar.2022.05.006
- SM. Hosseini, M. Mohammadi, O. Guerra-Santin, Interactive kinetic façade: Improving visual comfort based on dynamic daylight and occupant's positions by 2D and 3D shape changes, Building and Environment 165 (2019) 106396. https://doi.org/10.1016/j.buildenv.2019.106396
- D. Powell, I. Hischier, P. Jayathissa, B. Svetozarevic, A. Schlüter, A reflective adaptive solar façade for multi-building energy and comfort management, Energy and Buildings 177 (2018) 303-315. https://doi.org/10.1016/j.enbuild.2018.07.040
- H. Sarmadi, M. Mahdavinejad, A designerly approach to Algae-based large open office curtain wall Façades to integrated visual comfort and daylight efficiency, Solar Energy 251 (2023) 350-365. https://doi.org/10.1016/j.solener.2023.01.021
- R. M. ElBatran, WSE. Ismaeel, Applying a parametric design approach for optimizing daylighting and visual comfort in office buildings, Ain Shams Engineering Journal 12(3) (2021) 3275-3284. https://doi.org/10.1016/j.asej.2021.02.014
- M. Rastegari, S. Pournaseri, H. Sanaieian, Analysis of daylight metrics based on the daylight autonomy (DLA) and lux illuminance in a real office building atrium in Tehran, Energy 263 (2023) 125707. https://doi.org/10.1016/j.energy.2022.125707
- YH. Teo,JH. Yap, H. An, N. Xie, J. Chang, SCM. Yu, A simulation-aided approach in examining the viability of passive daylighting techniques on inclined windows, Energy and Buildings 282 (2023) 112739. https://doi.org/10.1016/j.enbuild.2022.112739
- Y. Hu, Q. Xue, H. Wang, P. Zou, J. Yang, S. Chen, Experimental investigation on indoor daylight environment of building with Cadmium Telluride photovoltaic window, Energy and Built Environment (2023). https://doi.org/10.1016/j.enbenv.2023.01.001
- D-K. Bui, TN. Nguyen, A. Ghazlan, N-T. Ngo, TD. Ngo, Enhancing building energy efficiency by adaptive façade: A computational optimization approach, Applied Energy 265 (2020) 114797. https://doi.org/10.1016/j.apenergy.2020.114797
- H. Kim, M.J. Clayton, Parametric behavior maps: A method for evaluating the energy performance of climate-adaptive building envelopes, Energy and Buildings 219 (2020) 110020. https://doi.org/10.1016/j.enbuild.2020.110020
- HH. Alzoubi, SM. Al-Rqaibat, The effect of hospital design on indoor daylight quality in children section in King Abdullah University Hospital, Jordan, Sustainable Cities and Society 14 (2015) 449-455. https://doi.org/10.1016/j.scs.2014.08.008
- E. Bingham, D. Whitaker, C. Farnsworth, J. Smith, Evidence-Based Design in Hospital Renovation Projects: Design Implementation for Patient Privacy and Comfort, Journal of Architectural Engineering 28(2) (2022) 04022002. https://doi.org/10.1061/(ASCE)AE.1943-5568.0000530
- ERCM. Huisman, E. Morales, J. van Hoof, HSM Kort, Healing environment: A review of the impact of physical environmental factors on users, Building and Environment 58 (2012) 70-80. https://doi.org/10.1016/j.buildenv.2012.06.016
- JH. Choi, Study of the relationship between indoor daylight environments and patient average length of stay (ALOS) in healthcare facilities, 2007, Texas A&M University available at: https://hdl.handle.net/1969.1/4755.
- MY. Park, C-G. Chai, H-K. Lee, H. Moon, JS. Noh, The Effects of Natural Daylight on Length of Hospital Stay, Environmental Health Insights 12 (2018) 1178630218812817. https://doi.org/10.1177/1178630218812817
- IP. Gradiški, P. Bilić, T. Sabo, M. Vilibić, Tracking insomnia seasonal variations through consumption of hypnotics, European Psychiatry 41 (2017) S283. https://doi.org/10.1016/j.eurpsy.2017.02.134
- A. Aguglia, G. Serafini, P. Solano, G. Giacomini , C. Conigliaro, V. Salvi, The role of seasonality and photoperiod on the lethality of suicide attempts: A case-control study, Journal of Affective Disorders 246 (2019) 895-901. https://doi.org/10.1016/j.jad.2018.12.094
- V. Heboyan, S. Stevens, W.V. McCall, Effects of seasonality and daylight savings time on emergency department visits for mental health disorders, The American Journal of Emergency Medicine 37(8) (2019) 1476-1481. https://doi.org/10.1016/j.ajem.2018.10.056
- M. Canazei, W. Pohl, J. Weninger, H. Bliem, EM. Weiss, C. Koch, Effects of adjustable dynamic bedroom lighting in a maternity ward, Journal of Environmental Psychology 62 (2019) 59-66. https://doi.org/10.1016/j.jenvp.2019.01.010
- M. Engwall, I. Fridh, L. Johansson, I. Bergbom, B. Lindahl, Lighting, sleep and circadian rhythm: An intervention study in the intensive care unit, Intensive and Critical Care Nursing 31(6) (2015) 325-335. https://doi.org/10.1016/j.iccn.2015.07.001
- L. Jin, NR. Ziebarth, Sleep, health, and human capital: Evidence from daylight saving time, Journal of Economic Behavior & Organization 170 (2020) 174-192. https://doi.org/10.1016/j.jebo.2019.12.003
- I. Kriszbacher, J Bódis, I. Boncz, A. Koppan, M. Koppan, The time of sunrise and the number of hours with daylight may influence the diurnal rhythm of acute heart attack mortality, International Journal of Cardiology 140(1) (2010) 118-120. https://doi.org/10.1016/j.ijcard.2008.11.019
- M. Meriläinen, H. Kyngäs, T. Ala-Kokko, 24-Hour intensive care: An observational study of an environment and events. Intensive and Critical Care Nursing 26(5) (2010) 246-253. https://doi.org/10.1016/j.iccn.2010.06.003
- A. Eijkelenboom, DH. Kim, PM. Bluyssen, First results of self-reported health and comfort of staff in outpatient areas of hospitals in the Netherlands, Building and Environment 177 (2020) 106871. https://doi.org/10.1016/j.buildenv.2020.106871
- SO. Sadegh, E. Gasparri, A. Brambilla, A. Globa, Kinetic facades: An evolutionary-based performance evaluation framework, Journal of Building Engineering 53 (2022) 104408. https://doi.org/10.1016/j.jobe.2022.104408
- A. Tabadkani, S. Banihashemi, M.R. Hosseini, Daylighting and visual comfort of oriental sun responsive skins: A parametric analysis, Building Simulation 11(4) (2018) 663-676. https://doi.org/10.1007/s12273-018-0433-0
- M. Wageh, M. Gadelhak, Optimization of Facade Design for Daylighting and View-to-Outside A case study in Lecco, Lombardy, Italy, 2017. https://doi.org/10.52842/conf.ecaade.2017.2.229
- A. Wagdy, A. Sherif, H. Sabry, R. Arafa, I. Mashaly, Daylighting simulation for the configuration of external sun-breakers on south oriented windows of hospital patient rooms under a clear desert sky, Solar Energy 149 (2017) 164-175. https://doi.org/10.1016/j.solener.2017.04.009
- AH. Sadek, R. Mahrous, Adaptive glazing technologies: Balancing the benefits of outdoor views in healthcare environments, Solar Energy 174 (2018) 719-727. https://doi.org/10.1016/j.solener.2018.09.032
- M. Boubekri, Daylighting, Architecture and Health, Elsevier, 2017. https://doi.org/10.1515/energyo.0106.00002
- H. Alzoubi, SA. Al-Rqaibat, RF. Bataineh, Pre-versus post-occupancy evaluation of daylight quality in hospitals, Building and Environment 45(12) (2010) 2652-2665. https://doi.org/10.1016/j.buildenv.2010.05.027
- J-H. Choi, L.O. Beltran, H-S. Kim, Impacts of indoor daylight environments on patient average length of stay (ALOS) in a healthcare facility, Building and Environment 50 (2012) 65-75. https://doi.org/10.1016/j.buildenv.2011.10.010
- A. Sherif, H. Sabry, R. Arafa, A. Wagdy, The Impact of Alternative Window Glazing Types and a Shading System on the Daylighting of Hospital Patient Rooms: Simulation Analysis under a Desert Clear Sky, Energy Procedia 78 (2015) 1805-1810. https://doi.org/10.1016/j.egypro.2015.11.315
- S. Cesari, P. Valdiserri, M. Coccagna, S. Mazzacane, Energy savings in hospital patient rooms: the role of windows size and glazing properties, Energy Procedia 148 (2018) 1151-1158. https://doi.org/10.1016/j.egypro.2018.08.027
- A. Sherif, H. Sabry, A. Wagdy, I. Mashaly, R. Arafa, Shaping the slats of hospital patient room window blinds for daylighting and external view under desert clear skies, Solar Energy 133 (2016) 1-13. https://doi.org/10.1016/j.solener.2016.03.053
- M. Englezou, A. Michael, Assessment of daylight performance and the impact of shading devices for typical in-patient rooms in healthcare facilities in Cyprus, Procedia Manufacturing 44 (2020) 277-285. https://doi.org/10.1016/j.promfg.2020.02.232
- N. Al-Shafaey, M. Abdelkader, H. Sabry, AA. Nessim, DOUBLE-SKIN FACADES IN HEALING ENVIRONMENTS: AN APPROACH FOR ENHANCING DAYLIGHTING PERFORMANCE IN SOUTH-ORIENTED PATIENT ROOMS IN CAIRO, EGYPT, Engineering Research Journal 165 (2020) 96-113. https://doi.org/10.21608/erj.2020.131829
- S. Alzubaidi, P. Soori, Energy Efficient Lighting System Design for Hospitals Diagnostic and Treatment Room-A Case Study, Journal of Light & Visual Environment 36 (2012) 23-31. https://doi.org/10.2150/jlve.36.23
- NJ. Kamali, MY. Abbas, Healing Environment: Enhancing Nurses' Performance through Proper Lighting Design, Procedia - Social and Behavioral Sciences 35 (2012) 205-212. https://doi.org/10.1016/j.sbspro.2012.02.080
- A. Nejati, S. Rodiek, M. Shepley, Using visual simulation to evaluate restorative qualities of access to nature in hospital staff break areas, Landscape and Urban Planning 148 (2016) 132-138. https://doi.org/10.1016/j.landurbplan.2015.12.012
- Y. Sun, Q. Huang, A Comparative Study of Design Strategies for Lobby of Outpatient Department of Hospital Buildings in Cold Climate Region in China, Procedia Engineering 180 (2017) 471-479. https://doi.org/10.1016/j.proeng.2017.04.206
- D. Greenberg, K. Pratt, B. Hencey, N. Jones, L. Schumann, J. Dobbs, Sustain: An experimental test bed for building energy simulation, Energy and Buildings 58 (2013) 44-57. https://doi.org/10.1016/j.enbuild.2012.11.026
- M. Sadeghipour Roudsari, M. Pak, Ladybug: A parametric environmental plugin for grasshopper to help designers create an environmentally-conscious design, in : 13th Conference of the International Building Performance Simulation Association, 2013: pp. 3128-3135. https://doi.org/10.26868/25222708.2013.2499
- F. Kharvari, An empirical validation of daylighting tools: Assessing radiance parameters and simulation settings in Ladybug and Honeybee against field measurements, Solar Energy 207 (2020) 1021-1036. https://doi.org/10.1016/j.solener.2020.07.054
- JW. Strunge, Building performance simulation in architectural design, in : Advanced Building Skins Conference, 2017, Bern.
- Weather data, EnergyPlus. https://energyplus.net/weather.
- CF. Reinhart, J. Mardaljevic, Z. Rogers, Dynamic Daylight Performance Metrics for Sustainable Building Design, LEUKOS 3 (2006) 7-31 . https://doi.org/10.1582/LEUKOS.2006.03.01.001
- M. Ayoub, 100 Years of daylighting: A chronological review of daylight prediction and calculation methods, Solar Energy 194 (2019) 360-390. https://doi.org/10.1016/j.solener.2019.10.072
- USGBC, LEED v4 for BUILDING DESIGN AND CONSTRUCTION, in Indoor environmental quality, 2019, p. 160. Available at: https://www.usgbc.org/articles/indoor-environmental-quality-and-leed-v4
- A. Gharaveis, MM. Shepley, K. Gaines, The Role of Daylighting in Skilled Nursing Short-Term Rehabilitation Facilities, HERD: Health Environments Research & Design Journal 9(2) (2016) 105-118. https://doi.org/10.1177/1937586715607835
- R. Jafarifiroozabadi, M. Woo, A. Joseph, P. MacNaughton, S. Mihandoust, The effects of window blind positions and control on patients' hospital and care quality perception: A mediation and moderation analysis, Building and Environment 226 (2022) 109672. https://doi.org/10.1016/j.buildenv.2022.109672
Copyright © 2023 The Author(s). Published by solarlits.com.

3590
Total views
Citations
SHARE ON



